
Tweet
Having discussed trypanosomiasis in both its African and American forms, we turn now to the other kinetoplastid-induced disease, leishmaniasis.


Having discussed trypanosomiasis in both its African and American forms, we turn now to the other kinetoplastid-induced disease, leishmaniasis.
The Leishmania genus designates another group of flagellated protozoan parasites. These are also hemoflagellates and they are members of the kinetoplastids, along with the Trypanosoma. The kinetoplast that both of these genera share is the DNA that is bound up in the mitochondrion organelle. This organelle complex is believed to be the high-energy locus for flagellated motility. As such, these are critical cellular structures for both the Leishmania and Trypanosoma, and thus define the class to which they both belong.
Below is the now familiar depiction of different developmental forms of the kinetoplastids. This picture can again be used as a reference for this discussion of the Leishmania life cycle:

The Leishmania do not share the last two forms, epimastigotes and trypomastigotes, with the Trypanosoma and so the Leishmania do not have an undulating membrane connecting to their flagella.
There are many species in the Leishmania genus (over three score), but not all are relevant to human infection. There are several species, that do infect humans, but only about 5 that are of primary importance to human transmission and subsequent disease. These major five are, Leishmania tropica, L. major, L. braziliensis, L. donovani, and L. infantum chagasi. These species have different geographic distributions, different vectors based on unique geography, and different manifestations of disease. All this detail will be discussed below. But first, let us discuss a generalized life-cycle of Leishmania spp. The Centers for Disease Control and Prevention (CDC) have created a nice graph demonstrating the life cycle of Leishmania species relevant to human infection:

As the sandfly vector takes its blood meal from the host, the Leishmania promastigotes are injected into the skin during the bite. The promastigotes are identified by innate immune surveillance and taken up by macrophages and dendritic cells during these cells' natural process of phagocytosis. Once inside the macrophages or dendritic cells, the promastigotes transform into amastigotes, which then multiply in the host cell. These amastigotes then rupture and exit the cell and are then able to infect new macrophages. Those Leishmania species that cause cutaneous disease remain at the site of infection, while those that cause mucocutaneous and visceral disease are able to migrate away from the site of infection to infect more distal locations. These distinct disease forms are described later in this post.
Those macrophages that are actively infected with amastigotes can also be taken up by, and infect, new sandflies during later blood meals. As the ingested macrophages are digested in the gut of the sandfly, the amastigotes are released and transform into promastigotes in the midgut. These promastigotes then divide in the midgut and migrate to the sandfly's proboscis, where they are poised to infect a new human host with the sandfly's next blood meal. Here is a picture of the promastigotes:

Once the Leishmania are taken up by their vertebrate host cells they become intracellular parasites, similar to Trypanosoma cruzi, which is the parasite that causes Chagas disease as discussed in the last posting. Subsequent amastigote generations are taken up by macrophages and, in the case of those species that cause visceral leishmaniasis, can be distributed far and wide throughout the host. The critical feature of this latter infection is that the parasites are able to co-opt the immune system. The Leishmania are able to not only evade the lysosomal and phagocytic activity of the macrophages, but also co-opt the cellular apparatus of these cells to enhance the parasites' own proliferation, ultimately damaging and killing the cell. Considering that this organism has utilized one of the key mechanisms of its host's innate immunity, we have to recognize that this is an incredibly adapted parasite that has found a way to use the host's defense to its own advantage. Amazing. Biology finds that which works.

Leishmania tropica
Once the Leishmania are taken up by their vertebrate host cells they become intracellular parasites, similar to Trypanosoma cruzi, which is the parasite that causes Chagas disease as discussed in the last posting. Subsequent amastigote generations are taken up by macrophages and, in the case of those species that cause visceral leishmaniasis, can be distributed far and wide throughout the host. The critical feature of this latter infection is that the parasites are able to co-opt the immune system. The Leishmania are able to not only evade the lysosomal and phagocytic activity of the macrophages, but also co-opt the cellular apparatus of these cells to enhance the parasites' own proliferation, ultimately damaging and killing the cell. Considering that this organism has utilized one of the key mechanisms of its host's innate immunity, we have to recognize that this is an incredibly adapted parasite that has found a way to use the host's defense to its own advantage. Amazing. Biology finds that which works.
The sandfly is the vector required for Leishmania transmission to vertebrate hosts. Known collectively as Phlebotomines (i.e., of the subfamily Phlebotominae), there are two sandfly genera that are relevant to transmission: the Phlebotomus and the Lutzomyia. Phlebotomus spp. make up the "Old World" sandlies and are found in the Mediterranean, Southern Europe, Africa, the Middle East, Central Asia, and South Asia:

The Lutzomyia spp. are the "New World" sandflies and are found throughout the Americas:

Whether referring to Phlebotomus or Lutzomyia, the sandfly shares some ecologic commonalities with other arthropod vectors that we have covered previously at Infection Landscapes. For example, the sandfly is similar to all mosquito vectors we have covered in that blood meals are taken exclusively for the production of eggs and so only females take blood. Sandflies also share mammal, reptile and bird hosts with mosquito vectors. But there is a critical difference between the sandfly vector and mosquito vectors: sandflies do not require an aquatic environment to complete their life cycle. Females often lay their eggs in soils but can, and frequently do, oviposition in any location containing decaying organic material, rather than on, in, or above water. As such, the sandfly can find suitable habitat in sylvan or domestic communities.
Sandflies typically bite at night or in the dusky hours of sunset and sunrise, which is similar to culicine and anopheline mosquitoes, but different from the day-biting Aedes spp. Another distinction between the sandfly and mosquito vectors is the longer time required by the sandfly to complete the life cycle. The time to developmental completion from egg to adult sandfly can require a month to a month and a half.
Here is a general depiction of the different stages of the life cycle for all sandflies created by the Sand Fly and Leishmania Research Group at the Liverpool School of Tropical Medicine. The stages are as follows: the egg first, followed by the four instars of the larva, then the pupa, and finally the adult at the top of the picture:

But here is a critical factor in sandfly ecology: because the larvae are so tiny, and because they do not require water, the micro-niches available for sandfly larvae development are multitude and non-specific. This aspect of the sandly ecology presents two problems. First, because their life cycle allows for a high degree of generalization (as opposed to the water constraints that impose aquatic specialization on mosquito vectors), the sandflies can often find suitable habitat both inside and outside the human environment. While sandflies are often found in sandy areas, they are by no means limited to these areas. They are also especially at home in the cracks and crevices of mud-walled homes (a similarity, you will remember, shared with the reduviid vectors that transmit Chagas disease). Second, sandfly generalization and adaption to many different micro-landscapes makes vector control extremely difficult. There are no primary water sources that can be targeted for sandfly control as can be done with mosquitoes. Vector control is typically limited to insecticide spraying around the home, which does have some effect but does not target the larger population of sandflies.
Another interesting aspect of sandflies, is that they are weak fliers. As such, they tend to fly only short distances and, having reached a target, hop along the surface once they have arrived. They are not good at maintaining themselves airborne for flight beyond a couple meters, and they do not hover. These characteristics distinguish sandflies from other flies and from mosquitoes, both of which are typically very good at taking flight.
Let us now discuss the actual disease caused by the Leishmania parasites: leishmaniasis. To start, leishmaniasis is not one disease, but rather it is three. As is the case with most infectious diseases, these three forms differ by geography and landscape. I will break these down below.
Cutaneous leishmaniasis. This is the most common form of leishmaniasis. It is usually caused by L. major and L. tropica, which is transmitted by Phlebotomus sandflies, in the Old World. In this region, it occurs primarily in the Mediterranean, the Middle East, the African Sahel, Southern Europe, Central Asia, and South Asia. Here are 2 very good maps of the disease distribution by Leishmania species, which were produced by the World Health Organization (WHO):


Cutaneous leishmaniasis also does occur in the New World, but this distribution is discussed below with mucocutaneous leishmaniasis because, in the western hemisphere, these occur together and are caused by a different species of Leishmania.
The disease. Cutaneous lesihmaniasis first presents with a papule at the bite site of the sandfly. This papule will go on to develop an ulcer, often severe, that can take up to a year to heal. This ulcer often leaves a very noticeable scar, but beyond that, this form of disease is not associated with any more serious morbidity because the Leishmania remain at the site of infection throughout the course of infection:

Nevertheless, given the extensive scarring that can result after the ulcer heals, if the bite occurs on the face this form of disease can be cosmetically damaging, which itself can be psychologically detrimental.
Mucocutaneous leishmaniasis. This is a severely disfiguring type of cutaneous leishmaniasis found in tropical and sub-tropical South America, Central America, and parts of Mexico. It is caused by L. braziliensis and is transmitted by Luztomyia sandflies. Here is the distribution map produced by the WHO:

The disease. Mucocutaneous leishmaniasis is a variant of cutaneous leishmaniasis that is limited to the Western Hemisphere. This is essentially cutaneous leishmaniasis that involves the mucous membranes of the nasopharyngeal complex and, occasionally, the genitalia. In this form, the L. braziliensis parasites are able to migrate away from the site of infection, and ultimately involve the mucous membrane tissues. When mucocutaneous leishmaniasis is left untreated the nasal septum, lips, and soft palate can be completely destroyed:

When this advanced, asphyxiation due to airway collapse or secondary bacterial infection can often lead to death. Mucocutaneous leishmaniasis as advanced as that depicted in the picture above takes time to develop. It is a slow process, and one that is quite treatable. This underscores the reality that this neglected tropical disease is yet another unchecked condition of poverty. Those who can access and/or afford appropriate medical treatment do not go on to develop this kind of advanced mucocutaneous leishmaniasis.
Visceral leishmaniasis. This is the systemic leishmaniasis, which is typically fatal if not treated. It is found in both the Eastern and Western Hemispheres. It is most frequently caused by L. donovani in the Old World, and L. infantum chagasi in the New World. And, again, Phlebotomus sandflies transmit the Old World parasites and Lutzomyia sandflies transmit the New World parasites.. Here is the WHO map showing the global distribution:

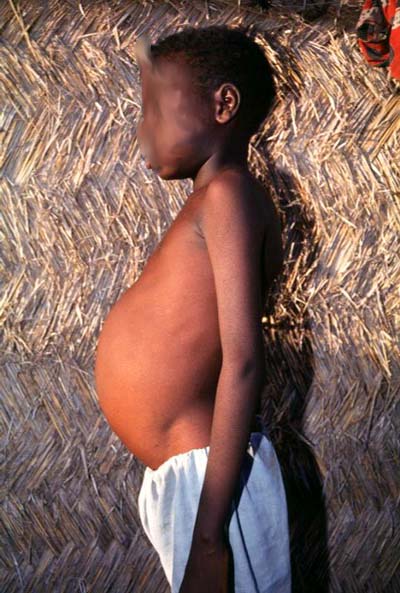
The disease. Visceral leishmaniasis, or kala-azar as it is known in many places by its India-derived name (meaning black fever), is pathologically and clinically quite distinct from the cutaneous leishmaniasis variants because the visceral form involves internal organs and carries the greatest associated mortality. In this form of disease, the Leishmania parasites are able to become far more dispersed throughout the host's reticuloendothelial system, whereas the cutaneous disease forms are much more localized, though L. braziliensis does migrate away from the site of infection in mucocutaneous leishmaniasis. In visceral leishmaniasis, the parasites are able to invade the spleen and liver, which causes a prolonged splenomegaly. The abdominal swelling of these organs is the most prominent clinical feature of this form of disease:

The greatest danger with visceral leishmaniasis is its impact on the immune system. After prolonged infection, the host's immune system deteriorates because these parasites directly attack the reticuloendothelial system. As such, people with visceral leishmaniasis become increasingly susceptible to other infections.
The descriptive epidemiology of leishmaniasis, in any form, is not good. This is due to poor surveillance, as was the case with both African and American trypanosomiasis. These diseases share several factors in common that preclude strong surveillance programs: they are largely rural diseases, they are diseases of the poor, and they fall into the general category of neglected tropical diseases.
Nevertheless we do have some estimates by way of the WHO. There are approximately 10 million people currently infected with one of the three forms of leishmaniasis discussed above. Depending on who is doing the estimating, worldwide there are anywhere between 500,000 and 2 million new cases of leishmaniasis per year, again including all forms. Truly staggering is the number of people who are potentially at risk: 300 million people live in leishmaniasis endemic areas and are currently at risk for infection.

Phlebotomus sp.

Lutzomyia longipalpis
Whether referring to Phlebotomus or Lutzomyia, the sandfly shares some ecologic commonalities with other arthropod vectors that we have covered previously at Infection Landscapes. For example, the sandfly is similar to all mosquito vectors we have covered in that blood meals are taken exclusively for the production of eggs and so only females take blood. Sandflies also share mammal, reptile and bird hosts with mosquito vectors. But there is a critical difference between the sandfly vector and mosquito vectors: sandflies do not require an aquatic environment to complete their life cycle. Females often lay their eggs in soils but can, and frequently do, oviposition in any location containing decaying organic material, rather than on, in, or above water. As such, the sandfly can find suitable habitat in sylvan or domestic communities.
Sandflies typically bite at night or in the dusky hours of sunset and sunrise, which is similar to culicine and anopheline mosquitoes, but different from the day-biting Aedes spp. Another distinction between the sandfly and mosquito vectors is the longer time required by the sandfly to complete the life cycle. The time to developmental completion from egg to adult sandfly can require a month to a month and a half.
Here is a general depiction of the different stages of the life cycle for all sandflies created by the Sand Fly and Leishmania Research Group at the Liverpool School of Tropical Medicine. The stages are as follows: the egg first, followed by the four instars of the larva, then the pupa, and finally the adult at the top of the picture:

But here is a critical factor in sandfly ecology: because the larvae are so tiny, and because they do not require water, the micro-niches available for sandfly larvae development are multitude and non-specific. This aspect of the sandly ecology presents two problems. First, because their life cycle allows for a high degree of generalization (as opposed to the water constraints that impose aquatic specialization on mosquito vectors), the sandflies can often find suitable habitat both inside and outside the human environment. While sandflies are often found in sandy areas, they are by no means limited to these areas. They are also especially at home in the cracks and crevices of mud-walled homes (a similarity, you will remember, shared with the reduviid vectors that transmit Chagas disease). Second, sandfly generalization and adaption to many different micro-landscapes makes vector control extremely difficult. There are no primary water sources that can be targeted for sandfly control as can be done with mosquitoes. Vector control is typically limited to insecticide spraying around the home, which does have some effect but does not target the larger population of sandflies.
Another interesting aspect of sandflies, is that they are weak fliers. As such, they tend to fly only short distances and, having reached a target, hop along the surface once they have arrived. They are not good at maintaining themselves airborne for flight beyond a couple meters, and they do not hover. These characteristics distinguish sandflies from other flies and from mosquitoes, both of which are typically very good at taking flight.
Let us now discuss the actual disease caused by the Leishmania parasites: leishmaniasis. To start, leishmaniasis is not one disease, but rather it is three. As is the case with most infectious diseases, these three forms differ by geography and landscape. I will break these down below.
Cutaneous leishmaniasis. This is the most common form of leishmaniasis. It is usually caused by L. major and L. tropica, which is transmitted by Phlebotomus sandflies, in the Old World. In this region, it occurs primarily in the Mediterranean, the Middle East, the African Sahel, Southern Europe, Central Asia, and South Asia. Here are 2 very good maps of the disease distribution by Leishmania species, which were produced by the World Health Organization (WHO):

Old World cutaneous leishmaniasis distribution due to L. major

Old World cutaneous leishmaniasis distribution due to L. tropica and L. aethiopica
Cutaneous leishmaniasis also does occur in the New World, but this distribution is discussed below with mucocutaneous leishmaniasis because, in the western hemisphere, these occur together and are caused by a different species of Leishmania.
The disease. Cutaneous lesihmaniasis first presents with a papule at the bite site of the sandfly. This papule will go on to develop an ulcer, often severe, that can take up to a year to heal. This ulcer often leaves a very noticeable scar, but beyond that, this form of disease is not associated with any more serious morbidity because the Leishmania remain at the site of infection throughout the course of infection:

Nevertheless, given the extensive scarring that can result after the ulcer heals, if the bite occurs on the face this form of disease can be cosmetically damaging, which itself can be psychologically detrimental.
Mucocutaneous leishmaniasis. This is a severely disfiguring type of cutaneous leishmaniasis found in tropical and sub-tropical South America, Central America, and parts of Mexico. It is caused by L. braziliensis and is transmitted by Luztomyia sandflies. Here is the distribution map produced by the WHO:

New World cutaneous and mucocutaneous leishmaniasis distribution
The disease. Mucocutaneous leishmaniasis is a variant of cutaneous leishmaniasis that is limited to the Western Hemisphere. This is essentially cutaneous leishmaniasis that involves the mucous membranes of the nasopharyngeal complex and, occasionally, the genitalia. In this form, the L. braziliensis parasites are able to migrate away from the site of infection, and ultimately involve the mucous membrane tissues. When mucocutaneous leishmaniasis is left untreated the nasal septum, lips, and soft palate can be completely destroyed:

When this advanced, asphyxiation due to airway collapse or secondary bacterial infection can often lead to death. Mucocutaneous leishmaniasis as advanced as that depicted in the picture above takes time to develop. It is a slow process, and one that is quite treatable. This underscores the reality that this neglected tropical disease is yet another unchecked condition of poverty. Those who can access and/or afford appropriate medical treatment do not go on to develop this kind of advanced mucocutaneous leishmaniasis.
Visceral leishmaniasis. This is the systemic leishmaniasis, which is typically fatal if not treated. It is found in both the Eastern and Western Hemispheres. It is most frequently caused by L. donovani in the Old World, and L. infantum chagasi in the New World. And, again, Phlebotomus sandflies transmit the Old World parasites and Lutzomyia sandflies transmit the New World parasites.. Here is the WHO map showing the global distribution:

Old and New World visceral leishmaniasis distribution
The disease. Visceral leishmaniasis, or kala-azar as it is known in many places by its India-derived name (meaning black fever), is pathologically and clinically quite distinct from the cutaneous leishmaniasis variants because the visceral form involves internal organs and carries the greatest associated mortality. In this form of disease, the Leishmania parasites are able to become far more dispersed throughout the host's reticuloendothelial system, whereas the cutaneous disease forms are much more localized, though L. braziliensis does migrate away from the site of infection in mucocutaneous leishmaniasis. In visceral leishmaniasis, the parasites are able to invade the spleen and liver, which causes a prolonged splenomegaly. The abdominal swelling of these organs is the most prominent clinical feature of this form of disease:
The greatest danger with visceral leishmaniasis is its impact on the immune system. After prolonged infection, the host's immune system deteriorates because these parasites directly attack the reticuloendothelial system. As such, people with visceral leishmaniasis become increasingly susceptible to other infections.
The descriptive epidemiology of leishmaniasis, in any form, is not good. This is due to poor surveillance, as was the case with both African and American trypanosomiasis. These diseases share several factors in common that preclude strong surveillance programs: they are largely rural diseases, they are diseases of the poor, and they fall into the general category of neglected tropical diseases.
Nevertheless we do have some estimates by way of the WHO. There are approximately 10 million people currently infected with one of the three forms of leishmaniasis discussed above. Depending on who is doing the estimating, worldwide there are anywhere between 500,000 and 2 million new cases of leishmaniasis per year, again including all forms. Truly staggering is the number of people who are potentially at risk: 300 million people live in leishmaniasis endemic areas and are currently at risk for infection.